IPFJES Site Initiation Visit
Dr Carl Reynolds and Miss Rupa Sisodia
Idiopathic Pulmonary Fibrosis Job Exposures Study
this talk is available online
this studies documentation is available online
Today we will cover why, what, and how
Why are we doing IPF JES?
- It's bad to not know the cause of a killer disease that is becoming more common
- There is ongoing asbestos exposure globally (including the UK)
- There is reason to think some IPF is due to asbestos, potentially we can better understand and prevent IPF
IPF causes significant morbidity and mortality
- c.4000 deaths in 2012 for England & Wales
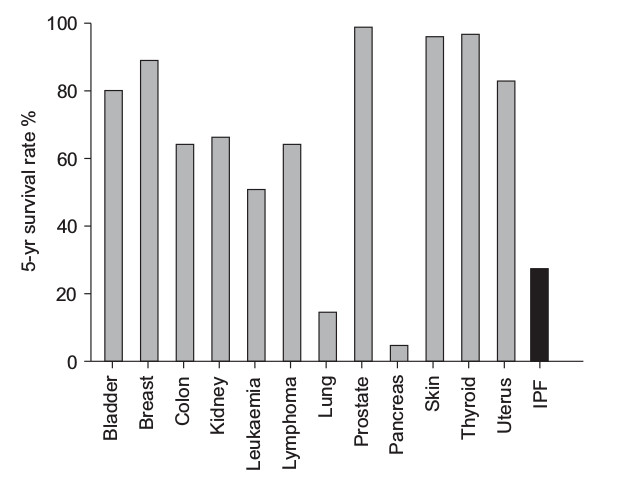
- median survival of three years; worse than several cancers
- more common in men, manual workers, those living in industrial regions
- incidence increasing 5% pa since 2000; don't know why
Asbestos related disease remains a problem
- 2 million metric tons per year of asbestos consumed per year
- 125 million people around the world work in environments in which they are exposed to asbestos
- 107,000 people die from occupational exposure to asbesotos / year
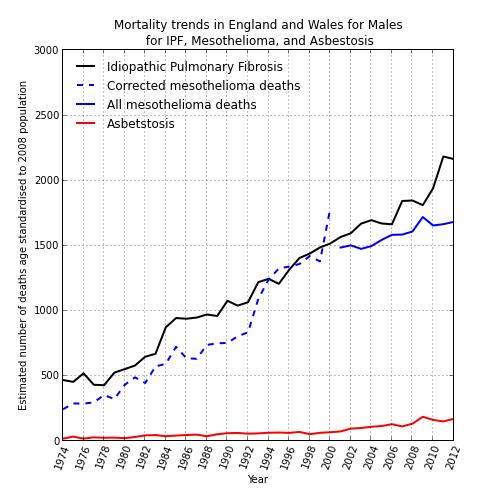
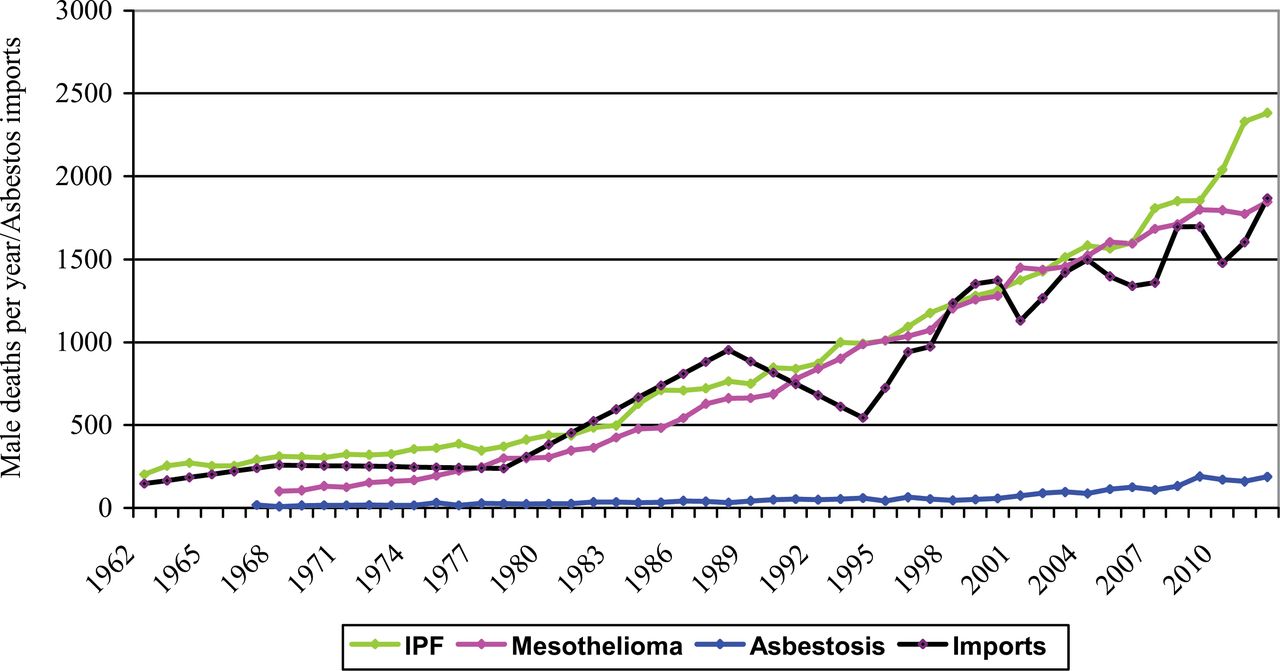
There is reason to think some IPF is due to asbestos
- Clinical Plausibility
- Observed epidemiological patterns
- Fibre studies and existing case-control data
- Clinical presentation can be similar
- Radiologically and histopathologically both give rise to UIP - no differentiating biomarkers
- Doctors may not elicit previous asbestos exposure and patients may not recall it; unclear what dose is needed
Previous studies
- 14 case-control studies to date
- 8 find an association with metal dust; 4 with wood; 2 with stone
- Most use community controls and self-reported exposure measures; none quantify asbestos exposure
- Occupational overlap with mesothelioma case-control studies
- (meta-analysis and analysis of occupational data from Navaratnams 2014 study - unpublished)
What we're doing
- (another) hospital-based case-control study
- lifetime occupational histories combined with occupational proportionate mortality ratios for mesothelioma and a job-process based asbestos exposure assessment..
- blood test for susceptibility genetics to investigate gene-exposure interactions
- basically a telephone-interview + blood test for 920 patients at 16 centres
How IPF JES works
- Funded by Wellcome Trust and in the NIHR portfolio. All regulatory approvals in place.
- Central research team: full-time clinical research fellow + research assistant, supervised by Prof Cullinan, Chris Barber, and Sara De Matteis. Advisory board of the great and the good. Study management and coordination + one site locally.
- Local research centres: PI + research nurse. Identification and recruitment of cases and controls.
- All the study documents are online https://github.com/drcjar/ipfjes/blob/master/README.md
Local centres identify and recruit participants
Key documents && events
- The SOP
- The bundle
- The box with blood and CRF
- The email(to ) with name and research ID (six digits long, centre ID plus unique identifier)
What's in the SOP
- how to identify cases and controls
- how to recruit them
- how to record the process and communicate with us
identifying cases and controls
- men with an incident diagnosis of IPF from Feb 2017 - Oct 2019 from the ILD clinic
- (age-matched) men without a diagnosis of IPF from not-the-ILD-Clinic
- never worked abroad (does not include armed services and merchant navy)
Selecting not-the-ILD-Clinic
- randomly selected
- using a list of all clinics / services / consultants / clinic locations and times
- we're not rigid about how as long as it's 'fair', we're happy to support
- local team asks the clinic lead if its ok to recruit from their clinic, if it's not then we select again
Recruiting cases (and controls) from clinic
- Provide participant information (using participant information sheet
- Obtain consent and signed consent form. Give patient the jobs sheet.
- Complete case-report form for participants + take or arrange blood sample collection (labelling both with participant research ID)
- Post case-report form and blood samples to us in the provided prepaid Royal Mail specimen bo:
- Email us () the participant esearch ID and name for the samples you're sending to us
on research IDs
- used to label samples and the CRF
- together with recruitment and tissue tracking clinic email allows us to telephone people
- six integers, first two integers identify centre, remaining four integers allocated however you like (as long as no duplicates)
on site files and logging
- we provide a local site file template
- (among other things) it's important to keep a recruitment screening log
What's in the bundle
- participant information sheet (contains enough information for a competent person to consent someone for the study)
- consent form
- case report form
- job history sheet